Leukopenia refers to a condition in which the total white blood cell count in the peripheral blood of adults persistently falls below 4.0×109/L. Neutropenia is defined as an absolute neutrophil count (ANC) in the peripheral blood that is less than 2.0×109/L in adults, less than 1.8×109/L in children aged ≥10 years, or less than 1.5×109/L in children under 10 years of age. When the absolute neutrophil count is below 0.5×109/L, the condition is referred to as agranulocytosis.
Etiology and Pathogenesis
The bone marrow is the sole site of neutrophil production and can be divided into the proliferative pool and the maturation storage pool. Adults produce approximately 1×109/kg of neutrophils daily, with about 90% stored in the bone marrow and approximately 10% released into peripheral blood. Of those entering the peripheral blood, about half circulate in the bloodstream (circulating pool), while the other half adhere to the walls of small blood vessels (marginal pool). These two pools exchange freely, maintaining dynamic equilibrium. Neutrophils remain in circulation for approximately 6–7 hours before migrating into tissues or inflammatory sites, where they are cleared by programmed cell death and macrophage phagocytosis.
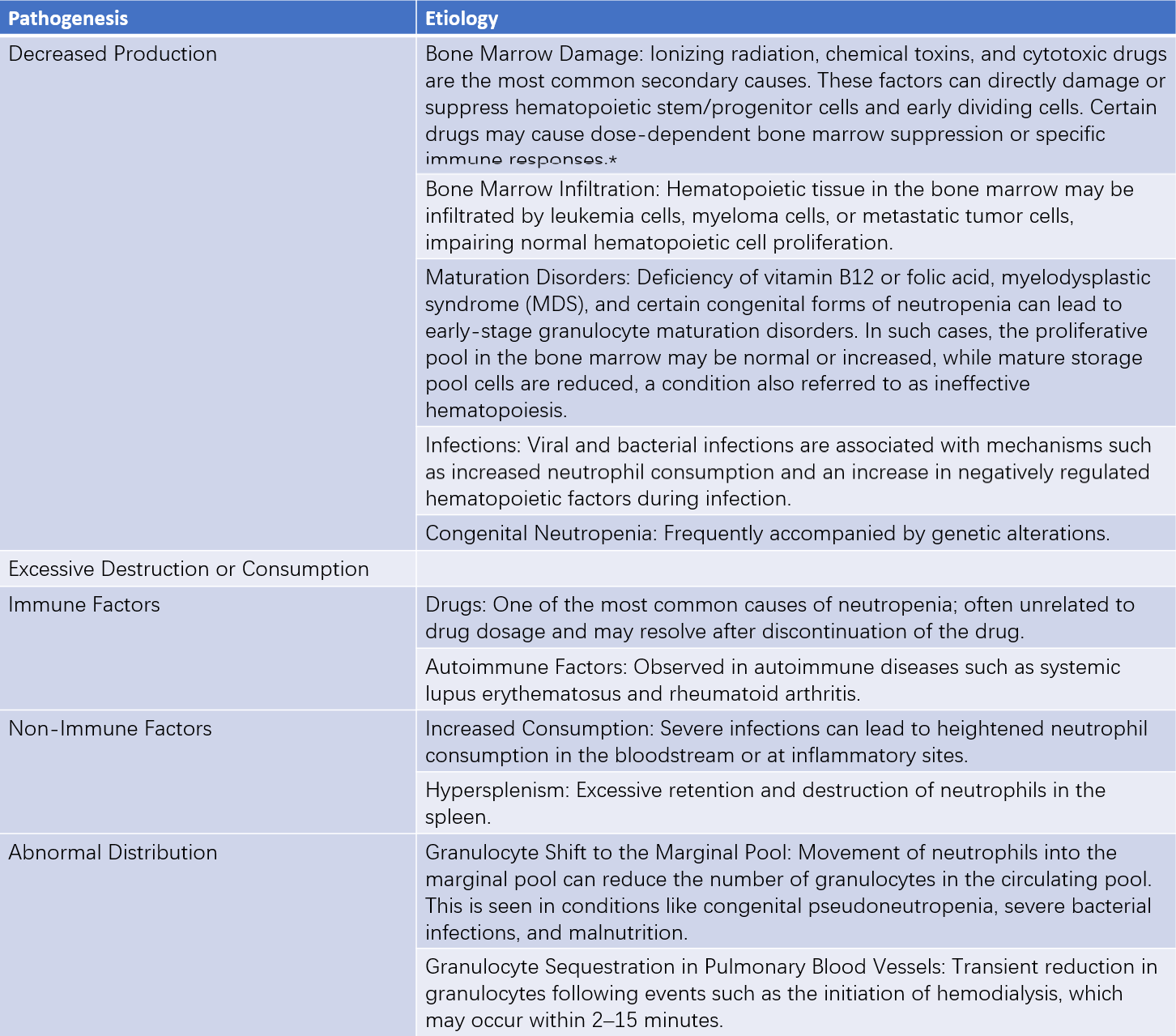
Table 1 Etiology and pathogenesis of neutropenia
Note: *Common drugs associated with leukopenia include cytotoxic antineoplastic drugs (alkylating agents, antimetabolites, etc.), antipyretic and anti-inflammatory drugs (aminopyrine, ibuprofen, etc.), antibiotics (chloramphenicol, penicillin, sulfonamides, etc.), antituberculosis drugs (isoniazid, rifampin, etc.), antimalarial drugs (chloroquine, primaquine, etc.), antithyroid drugs (methimazole, propylthiouracil, etc.), hypoglycemic agents (tolbutamide, etc.), anticonvulsants/antiepileptic drugs (phenytoin, phenobarbital, etc.), antihypertensive drugs (captopril, etc.), immunomodulators (azathioprine, mycophenolate mofetil, etc.), and antipsychotic drugs (chlorpromazine, etc.).
The causes of neutropenia can be congenital or acquired, with the latter being more common. Based on cellular dynamics, the etiology and pathogenesis of neutropenia can be categorized into three main types: reduced production, excessive destruction or consumption, and abnormal distribution. In adults, the primary causes of neutropenia are decreased production and autoimmune destruction, while abnormal distribution is rarely seen.
Clinical Manifestations
The clinical manifestations of neutropenia vary depending on its severity and the underlying cause. Neutropenia can be classified into mild (>1.0×109/L), moderate (0.5–1.0×109/L), and severe (<0.5×109/L). In cases of mild neutropenia, the risk of infection is low, and no specific symptoms are usually observed. Moderate to severe neutropenia increases susceptibility to infections, particularly in cases of severe neutropenia with prolonged duration, where serious infections may develop. Patients may present with symptoms such as chills and high fever.
The most commonly affected sites are the respiratory tract, gastrointestinal tract, and urinary tract. In severe cases, septicemia and septic shock can occur. When neutrophils are profoundly absent, the infection site may fail to generate an effective inflammatory response, often resulting in little or no pus. For example, pulmonary infections might not show inflammatory infiltration on X-ray imaging.
Laboratory Examinations
Routine Tests
Routine blood tests typically reveal leukopenia and neutropenia, with an increased percentage of lymphocytes. The bone marrow findings vary depending on the underlying cause of neutropenia.
Specialized Tests
Determination of neutrophil-specific antibodies assists in identifying autoimmune neutropenia.
The epinephrine test mobilizes neutrophils from the marginal pool into the circulating pool, helping to distinguish pseudoneutropenia.
The hydrocortisone test assesses bone marrow granulocyte reserve.
For patients who experience early onset, recurrent infections, or have a family history of congenital neutropenia or congenital bone marrow failure syndromes, second-generation sequencing may be performed.
Diagnosis and Differential Diagnosis
Diagnosis of leukopenia, neutropenia, or agranulocytosis can be made based on the results of a complete blood count. It is important to exclude errors in testing techniques, normal physiological factors (e.g., exercise, pregnancy, seasonal variations), age, race, and blood sampling site. Re-evaluation, including peripheral blood cell morphology analysis, may sometimes be necessary.
Differentiating the etiology of neutropenia is crucial for treatment. Key considerations include assessing a history of exposure to medications, chemical agents, radiation, or chemotherapy, as well as any history of infectious diseases, autoimmune disorders, and neoplastic conditions. Other factors, such as the age of onset, severity, rate of progression, duration, periodicity, the presence of underlying diseases, and family history, should also be investigated. If splenomegaly is present, hypersplenism should be considered.
Treatment
Etiological Treatment
For suspected drugs or other causative factors, cessation of exposure is necessary. In cases of secondary neutropenia, addressing the underlying disease is critical. Granulocyte levels can return to normal after remission or control of the primary condition.
Infection Prevention and Control
Mild neutropenia generally does not require pharmacological treatment. For moderate neutropenia, the infection risk is elevated, and precautions such as avoiding crowded places, maintaining hygiene, and eliminating chronic infectious foci are recommended. Prophylactic use of antibiotics is not advised. Patients with agranulocytosis are highly susceptible to severe infections, requiring sterile isolation measures. Identification of febrile infection should involve pathogen testing to determine the infection type and site. Broad-spectrum antibiotics should be initiated empirically and adjusted based on pathogen and drug susceptibility results. Attention should also be given to preventing secondary infections, particularly fungal infections.
Promotion of Granulocyte Production
Recombinant human granulocyte colony-stimulating factor (rhG-CSF) and recombinant human granulocyte-macrophage colony-stimulating factor (rhGM-CSF) can enhance the proliferation, release, and functions of neutrophils, including phagocytosis, bactericidal activity, and chemotaxis. The typical dosage of rhG-CSF ranges from 2–10 μg/(kg·d). Common adverse effects of these treatments include fever, musculoskeletal pain, and rash. Indications and dosage of rhG-CSF vary depending on the cause of neutropenia.
Immunosuppressive Therapy
Autoimmune neutropenia and neutropenia caused by immune mechanisms can be treated with immunosuppressive agents such as glucocorticoids and cyclosporine.
Hematopoietic Stem Cell Transplantation
Hematopoietic stem cell transplantation is a curative treatment for conditions such as congenital agranulocytosis and bone marrow failure.
Prognosis
Prognosis depends on the severity, duration, progression, etiology of neutropenia, and the adequacy of treatment. Mild to moderate cases generally have a favorable prognosis if there is no progression. For agranulocytosis, mortality rates have decreased with the use of broad-spectrum antibiotics, but the prognosis still depends on the prompt removal of the causative factor.