Von Willebrand disease (vWD) is a commonly encountered autosomal hereditary bleeding disorder in clinical practice. Its inheritance pattern exhibits heterogeneity. The condition is characterized by a predisposition to bleeding from an early age, prolonged bleeding time, reduced platelet adhesion, defective ristocetin-induced platelet aggregation, and either a deficiency or structural abnormality of plasma von Willebrand factor (vWF) antigen. The prevalence is approximately 1–10 per 1,000 individuals. Acquired von Willebrand disease can arise secondary to various underlying conditions, although in some cases it may occur without any identifiable underlying disease.
Etiology and Pathogenesis
vWF primarily resides in endothelial cells, megakaryocytes, and platelets. Its main physiological functions include:
- Forming a non-covalent complex with FVIII, thereby increasing FVIII stability, preventing its degradation, and facilitating its generation and release.
- Acting as a critical bridge in the adhesion of platelets to the vessel wall. Upon platelet activation, one end of vWF binds to platelet glycoprotein Ib, while the other end binds to fibronectin and collagen in the injured vessel wall, securing platelet adhesion to the vascular endothelium.
The vWF gene is located at the terminal region of the short arm of chromosome 12. When gene defects occur, vWF production is reduced or its function becomes abnormal, accompanied by a decline in FVIII:C levels and impaired platelet adhesion and aggregation.
Various mechanisms underlie acquired von Willebrand disease. The most common cause is the production of inhibitors with anti-vWF activity, predominantly IgG. Other causes include adsorption of vWF by tumor cells, leading to reduced plasma vWF levels, or inhibitors binding to inactive regions of vWF to form complexes, which accelerates its destruction within the mononuclear phagocyte system.
Clinical Manifestations
The primary clinical manifestation is a bleeding tendency. Compared to hemophilia, bleeding in vWD exhibits the following characteristics:
- Predominantly affects the skin and mucosa, presenting as epistaxis, gingival bleeding, bruises, and bleeding after minor trauma or procedures, such as tooth extraction.
- Occurs in both males and females; female patients in adolescence may experience heavy menstrual bleeding and postpartum hemorrhage.
- Bleeding episodes may decrease in severity with age, potentially due to an age-related increase in vWF activity.
- Spontaneous joint or muscle bleeding is relatively rare, with fewer instances of disability resulting from such bleeding.
Laboratory Tests
Bleeding Screening Tests
Tests include complete blood count, activated partial thromboplastin time (APTT)/prothrombin time (PT), and plasma fibrinogen measurement. The results of screening tests are often normal or may show a prolonged APTT, which can usually be corrected with normal plasma.
Diagnostic Tests
These include plasma vWF antigen (vWF:Ag) measurement, plasma ristocetin cofactor activity of vWF (vWF:RCo), and plasma FVIII coagulation activity (FVIII:C) measurement. Abnormalities in one or more of these diagnostic tests necessitate further subtyping diagnostic tests.
Subtype Diagnostic Tests for vWD
These tests include:
- Plasma vWF multimer analysis.
- Ristocetin-induced platelet aggregation (RIPA).
- Plasma vWF collagen-binding activity assay (vWF:CB).
- Plasma vWF factor VIII binding activity measurement (vWF:FVIIIB).
For patients with a clear history of bleeding or a family history of bleeding disorders, a stepwise approach to performing these laboratory tests is recommended to confirm the diagnosis of vWD and exclude other bleeding-related disorders.
Diagnosis and Classification
Key Points for Diagnosis
A family history may or may not be present. In cases with a family history, inheritance usually follows an autosomal dominant or recessive pattern.
A history of spontaneous bleeding or excessive bleeding following trauma or surgery is usually consistent with the clinical manifestations of vWD.
Plasma vWF:Ag <30% and/or vWF:RCo <30%; FVIII:C <30% is observed in type 2N and type 3 vWD.
Exclusion of other conditions such as hemophilia, acquired vWD, platelet-type vWD, and inherited platelet disorders is essential.
Differential Diagnosis
The measurement of vWF:Ag differentiates vWD from hemophilia A and B. The assessment of platelet morphology distinguishes vWD from macrothrombocytopenia syndromes.
Classification
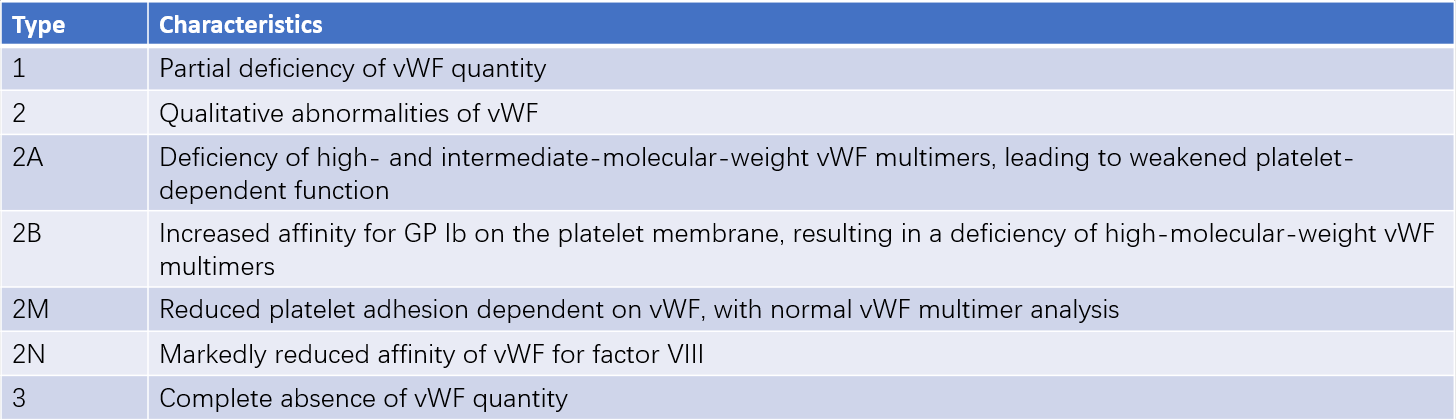
Based on the pathogenesis, vWD can be classified into three main types:
- Type 1 and Type 3 vWD are characterized by quantitative deficiencies of vWF.
- Type 2 vWD is characterized by qualitative defects in vWF.
- Type 2 vWD can be further subdivided into four subtypes: 2A, 2B, 2M, and 2N.
Table 1 Common subtypes of von Willebrand disease
Treatment
Hemostatic effects are achieved during bleeding episodes or the perioperative period by elevating plasma vWF levels, supplemented with other hemostatic agents. Treatment approaches are tailored to the vWD type and the characteristics of the bleeding episode. Preventive treatment can be considered for patients with recurrent severe joint or visceral bleeding.
Desmopressin (DDAVP)
Desmopressin works by stimulating endothelial cells to release stored vWF, thereby increasing plasma vWF levels. It is effective for type 1 vWD, partially effective for types 2A, 2M, and 2N, ineffective for type 3, and should be used with caution in type 2B. The recommended dose is 0.3 μg/kg, diluted in 30–50 mL of normal saline, administered via slow intravenous infusion (over at least 30 minutes). It can be repeated every 12–24 hours, although its efficacy decreases with repeated use. Side effects include facial flushing, headache, and tachycardia. Repeated use may result in water retention and hyponatremia, necessitating fluid restriction. Use in elderly patients with cardiovascular or cerebrovascular diseases requires caution.
Replacement Therapy
Replacement therapy is appropriate for all types of vWD during bleeding episodes or surgery and for patients unresponsive to DDAVP. Plasma-derived vWF-containing concentrates or recombinant vWF products are the treatment of choice. If unavailable, cryoprecipitate or fresh frozen plasma may be used, though these carry a risk of transmitting transfusion-related infections. Dosing depends on the type of vWD and the nature of the bleeding episode. Dosage calibration is based on the vWF:RCo or FVIII:C levels in the preparation.
Other Treatments
Antifibrinolytic Agents
Aminocaproic acid can be administered with an initial dose of 4–5 g via intravenous infusion, followed by 1 g/hour until bleeding is controlled, with a total daily dose not exceeding 24 g.
Tranexamic acid can be dosed at 10 mg/kg via intravenous infusion every 8 hours.
Antifibrinolytic agents carry a risk of thromboembolism and should not be used in patients with hematuria. They can be applied topically for gingival bleeding.
Topical Hemostatic Agents
Local application of thrombin or fibrin sealant can provide additional benefits in managing skin and mucosal bleeding.