The cochlear implant is an electronic device that functions as a sound-to-electricity converter, designed to restore or provide hearing for individuals with severe to profound sensorineural hearing loss or total deafness. It converts sound signals into electrical signals that directly stimulate spiral ganglion neurons and auditory nerve fibers, thereby generating auditory perception. After over 50 years of experimental research and clinical application, cochlear implants have evolved from single-channel to multi-channel designs, with continuous improvements in speech coding strategies. They are now widely used domestically and internationally for the treatment of severe, profound sensorineural hearing loss and deafness. In 1978, Clark successfully developed the first clinically applicable multi-channel cochlear implant, which was subsequently approved for use in both adults and children. China has also developed multi-channel cochlear implants with independent intellectual property rights, which are now widely applied in clinical practice.
The complete process of cochlear implantation involves preoperative evaluation, the implantation surgery, and postoperative rehabilitation including training in auditory and speech skills. Successful outcomes require collaboration between the patient, the surgeon, audiologists, speech rehabilitation professionals, and the patient's family members.
Basic Structure
The cochlear implant consists of:
- External components: Including a directional microphone, a speech signal processor, and a transmitter.
- Internal components: Including a receiver, a decoding unit, and stimulation electrodes.
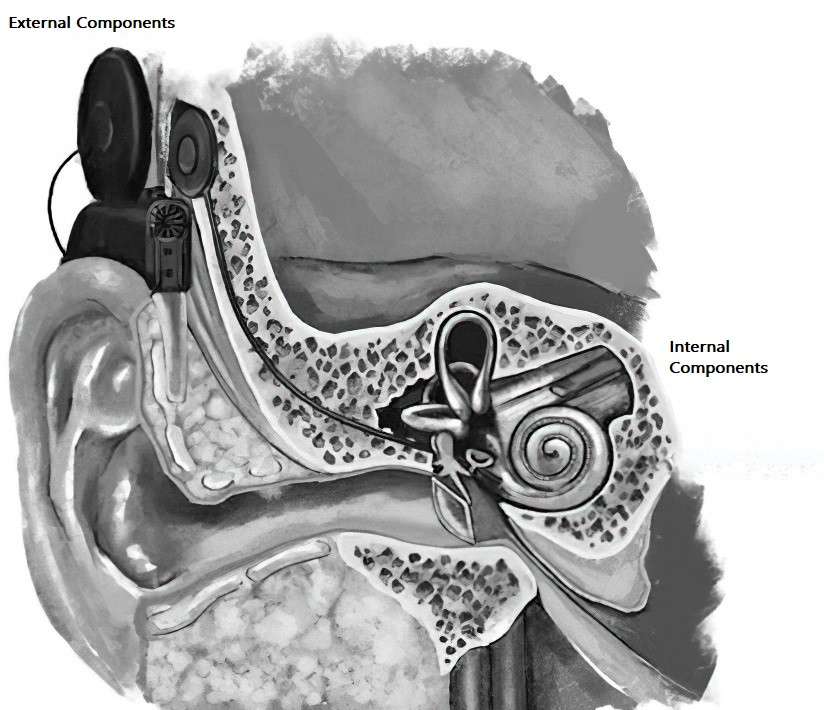
Figure 1 Basic structure of the cochlear implant
Basic Working Mechanism and Process
In a normal cochlea, sound waves are converted into bioelectrical signals by cochlear hair cells. The cochlear implant mimics this function by converting sound signals into electrical signals, which are transmitted to the cochlea via electrodes, replacing damaged hair cells to directly stimulate spiral ganglion neurons. The signals are then transmitted to the auditory central system, creating the perception of sound.
The basic working process involves:
- The external directional microphone capturing external sound signals.
- The sound signals being encoded by the speech processor.
- The encoded signals being transmitted via the external transmitting coil to the internal receiving coil, from where they are sent to the decoder and stimulation electrodes.
- The intracochlear stimulation electrodes generating electrical pulses, stimulating the residual spiral ganglion cells within the cochlea. These impulses are transmitted via the cochlear nerve to the auditory central pathways, leading to auditory perception.
Coding Strategies
The speech recognition performance after cochlear implantation is highly influenced by the speech coding strategy used. Over multiple generations of development, the most commonly adopted coding strategies currently include:
- SPEAK (Spectral Peak Extraction) Strategy
- CIS (Continuous Interleaved Sampling) Strategy
- ACE (Advanced Combination Encoder) Strategy
Most cochlear implant speech processors used in clinical practice incorporate two or three of these strategies, allowing for the selection of the most suitable coding scheme based on the specific needs of individual recipients.
Indications
Indications include:
- Patients with bilateral severe or profound sensorineural hearing loss or total deafness, including prelingual deafness and some cases of congenital deafness, whose auditory nerve integrity has been assessed. In such cases, hearing loss of ≥90 dB HL in both ears renders conventional hearing aids ineffective.
- Patients aged one year and older. Prelingual deafness patients are recommended to receive cochlear implants before the age of six, as research has shown that implantation during the early stages of language development (ages 0 to 6) significantly benefits the recovery of speech abilities. There is no age limit for postlingual deafness.
- Patients unable to improve their hearing and speech comprehension abilities with hearing aids or other assistive hearing devices.
- Patients who have a strong desire to improve their hearing, with a proper understanding of cochlear implants and reasonable expectations, expressed by the recipient and/or their guardians.
- Patients with the capacity to participate in postoperative speech rehabilitation plans. For children, this requires a comprehensive educational framework to support auditory and speech training after the procedure.
Candidates should have no contraindications for surgery.
Auditory and Speech Rehabilitation
Postoperative auditory and speech rehabilitation is critical, with the primary goal of helping recipients rebuild or improve their auditory and speech abilities while alleviating or mitigating psychological issues caused by auditory and speech impairments. For prelingual deafness patients, regardless of their actual age, their "auditory age" after cochlear implantation begins at zero. Postoperative auditory training, therefore, must follow a gradual and systematic progression.