Epidemiology
Chronic heart failure (CHF) is the final stage of cardiovascular disease and the leading cause of death. The prevalence of heart failure in adults is about 1% - 2%, and the overall prevalence is increasing. Both the incidence and prevalence of heart failure are rising. Coronary heart disease and hypertension have been the primary causes of chronic heart failure, and the most common is coronary heart disease, followed by hypertension. The proportion of rheumatic heart disease is decreasing, but with an aging population, the incidence of degenerative valvular disease is increasing, making valvular heart disease still significant. Additionally, chronic pulmonary heart disease and high-altitude heart disease have high regional prevalence.
Clinical Manifestations
Left Heart Failure
Left heart failure is characterized mainly by pulmonary congestion and reduced cardiac output.
Exertional dyspnea is the earliest symptom of left heart failure, caused by increased venous return during exercise, raising left atrial pressure and exacerbating pulmonary congestion. As heart failure progresses, exercise tolerance decreases.
Patients awaken suddenly due to breathlessness and are forced to sit up, and the symptoms are often relieved by sitting upright. This occurs due to increased pulmonary blood volume from blood redistribution while lying down, increased vagal tone at night, bronchial constriction, diaphragm elevation, and reduced lung capacity.
When pulmonary congestion reaches a certain level, patients cannot lie flat as venous return increases and the diaphragm rises, making breathing more difficult. Improvement occurs in high pillow position, semi-recumbent position, or orthopneic position.
Acute pulmonary edema is the most severe form of dyspnea in left heart failure, possibly accompanied by wheezing, known as cardiac asthma.
Cough and expectoration are caused by congestion of the alveoli and bronchial mucosa, often occurring at night and relieved when sitting or standing, and are characterized by white, serous, frothy sputum, occasionally blood-tinged. Acute left heart failure can produce pink, frothy sputum. Long-term chronic pulmonary congestion increases pulmonary venous pressure, forming collateral circulation between pulmonary and bronchial circulation under the bronchial mucosa, which can rupture and cause massive hemoptysis.
Malaise, lassitude, dizziness, and palpitations are symptoms due to insufficient organ and tissue perfusion and compensatory tachycardia.
Severe left heart failure leads to blood redistribution, reducing renal blood flow and causing oliguria. Long-term reduction in renal blood flow and increased renal venous pressure can result in symptoms of renal insufficiency.
Due to increased pulmonary capillary wedge pressure, fluid leaks into the alveoli, causing moist crackles. As the condition worsens, crackles can spread from the lung bases to the entire lung. More crackles are heard on the dependent side in lateral decubitus position.
In addition to the inherent signs of underlying heart disease, there may be cardiac enlargement, tachycardia, regurgitant murmur of relative mitral insufficiency, accentuated second heart sound in the pulmonary valve area, and gallop rhythms of the third or fourth heart sound.
Cyanosis is mainly due to edema and thickening of the respiratory membrane, impaired oxygen exchange, decreased partial pressure of oxygen, and increased reduced hemoglobin, and is classified as central cyanosis.
Right Heart Failure
Right heart failure is characterized mainly by systemic venous congestion.
Congestion in the gastrointestinal tract and liver causes abdominal distension, anorexia, nausea, and emesis, which are the most common symptoms of right heart failure.
Exertional dyspnea is more pronounced when secondary to lung disease and left heart failure. Isolated right heart failure can also cause exertional dyspnea, but patients can still be in recumbent position. This dyspnea is mainly due to decreased cardiac output and hypoxia, differing from the pulmonary congestion-induced dyspnea of left heart failure.
Malaise, lassitude, dizziness, and palpitations are mainly caused by reduced cardiac output, insufficient perfusion of tissues and organs, and compensatory tachycardia.
Increased systemic venous pressure causes edema in soft tissues, characterized by symmetrical pitting edema starting in dependent areas.
Enhanced jugular vein pulsation, distension, and engorgement are major signs of right heart failure; a positive hepatojugular reflux test is more characteristic.
Congestion and enlargement of the liver and spleen are often accompanied by tenderness; chronic right heart failure can lead to cardiac cirrhosis.
Serous cavity effusion can present pleural effusion, often bilateral, more pronounced on the right side, mainly due to increased pressures in both systemic and pulmonary circulation and increased pleural capillary permeability. Severe right heart failure can cause ascites due to obstructed hepatic venous return or concurrent cardiac cirrhosis.
In addition to signs of underlying heart disease, there may be tachycardia, right ventricular diastolic gallop rhythms, right heart enlargement, and regurgitant murmurs of relative tricuspid insufficiency.
Global Heart Failure
Global heart failure exhibits symptoms and signs of both left and right heart failure simultaneously. Most cases of global heart failure develop from left heart failure, where reduced right heart output decreases left heart preload, somewhat alleviating pulmonary congestion symptoms such as dyspnea. Cardiomyopathy and myocarditis can simultaneously affect both ventricles, presenting global heart failure from the onset.
Classification
According to the progression, heart failure can be divided into 4 stages.
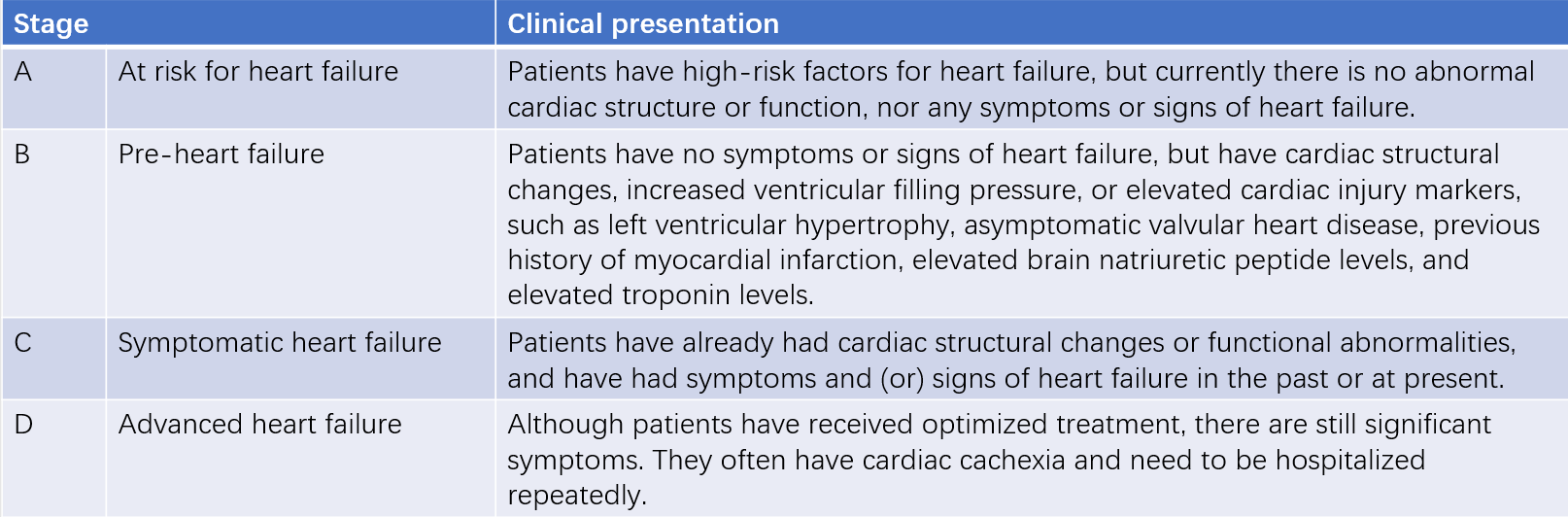
Table 1 Stages of chronic heart failure
According to the severity, heart failure can be divided into 4 classes.
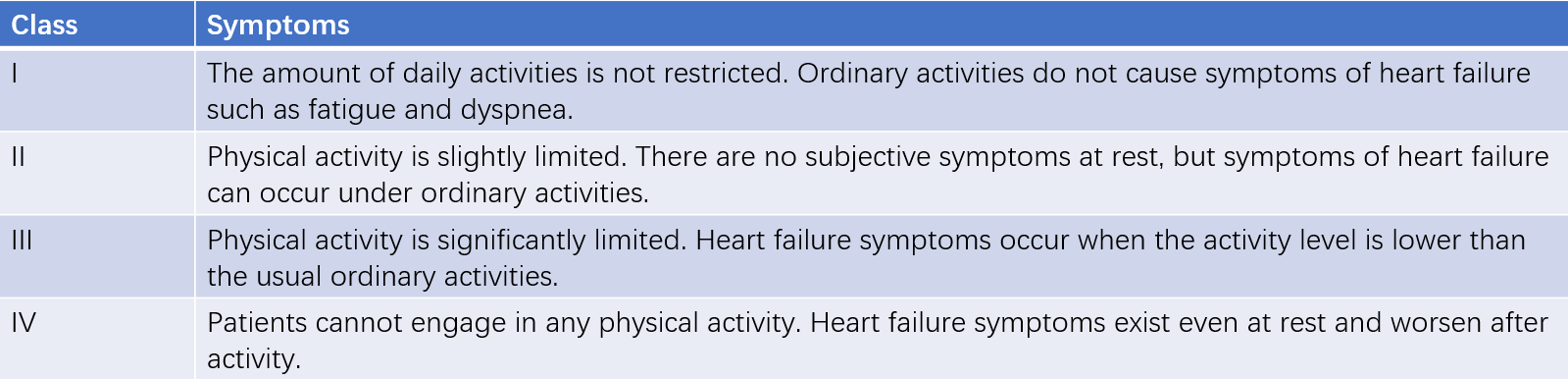
Table 2 Classes of cardiac function
Auxiliary Examinations
Laboratory Tests
B-type Natriuretic Peptide (BNP)
BNP is an important marker for the diagnosis, prognosis, and treatment evaluation of heart failure. Clinically, BNP and NT-proBNP are commonly used. Compared to BNP, NT-proBNP has a longer half-life and is more stable.
The sensitivity, specificity, negative predictive value, and positive predictive value of BNP for diagnosing heart failure are high. In patients with acute dyspnea, BNP/NT-proBNP has a high negative predictive value; normal levels can essentially rule out acute heart failure. BNP < 35 ng/L or NT-proBNP < 125 ng/L is typically used to exclude chronic heart failure, though the sensitivity and specificity are lower than for acute heart failure. Notably, about 20% of patients with heart failure with preserved ejection fraction (HFpEF) have normal BNP/NT-proBNP levels.
BNP levels are associated with heart failure prognosis; a decrease after treatment indicates improved prognosis.
BNP levels are influenced by age, gender, and weight, and are higher in older adults and females and lower in obese individuals. Left ventricular hypertrophy, tachycardia, myocardial ischemia, pulmonary embolism, renal insufficiency, infection, and sepsis can also elevate BNP levels.
Troponin
In patients with severe heart failure or decompensation, troponin levels may be slightly elevated. However, the primary purpose of measuring troponin in heart failure patients is to determine the presence of acute coronary syndrome. Elevated troponin, especially when accompanied by increased BNP, is a strong predictor of heart failure prognosis.
Routine Tests
Routine tests include complete blood count, urinalysis, liver and kidney function tests, electrolytes, thyroid function, serum ferritin concentration, and transferrin saturation.
Electrocardiogram (ECG)
Heart failure does not have specific ECG manifestations, but ECG can help assess myocardial ischemia and arrhythmias. It can also provide some treatment indications, such as anticoagulation therapy for atrial fibrillation, pacing for significant bradycardia, and cardiac resynchronization therapy for widened QRS complexes.
Imaging Examinations
Echocardiography
Echocardiography is the primary imaging test for diagnosing and evaluating heart failure, as it accurately assesses the size of heart chambers and the structure and function of valves, conveniently evaluates cardiac function, and aids in determining the etiology.
Key indicators of systolic function include ejection fraction (EF), fractional shortening, and circumferential fiber shortening velocity. EF is most used, and the modified biplane Simpson method is recommended. Although EF is not very precise, it is convenient and practical.
Doppler ultrasound is the most practical method for assessing diastolic function. Indicators include E/e', E/A, e', peak tricuspid regurgitation velocity, pulmonary artery systolic pressure (PASP), and global longitudinal strain (GLS). E/e' ≥ 15 can be used to diagnose HFpEF, while E/A < 1.2 suggests impaired diastolic function. When assessing diastolic dysfunction, morphological indicators such as left atrial volume index (LAVI), left ventricular mass index (LVMI), wall thickness, and relative wall thickness (RWT) should be considered.
Exercise or pharmacological stress echocardiography can be used for evaluating myocardial ischemia and certain valvular heart diseases, and diagnosing HFpEF.
Chest X-ray
Chest x-ray helps differentiate heart failure from lung diseases. The size and shape of the cardiac silhouette can provide important diagnostic clues, though not all heart failure patients have an enlarged cardiac silhouette.
Chest x-ray can reflect pulmonary congestion, including enhanced pulmonary vascular markings, increased upper lobe vascular markings, widened pulmonary arteries, interstitial pulmonary edema, Kerley B lines, butterfly opacities, and pleural effusion.
Cardiac Magnetic Resonance (CMR)
CMR's 3D imaging can overcome geometric assumptions in volume calculations, allowing precise measurement of end-systolic and end-diastolic ventricular volumes, EF, and stroke volume (SV). It offers excellent resolution for the right ventricle and complex congenital heart diseases. CMR also has high tissue resolution, and techniques such as late gadolinium enhancement (LGE) can distinguish ischemic changes from non-ischemic changes, assess myocardial fibrosis, and identify specific cardiomyopathies. CMR is recommended for suspected myocarditis, arrhythmogenic right ventricular cardiomyopathy (ARVC), cardiac amyloidosis, sarcoidosis, hemochromatosis, and diseases with undiagnosed etiologies.
Coronary Angiography (CAG)
In heart failure patients with coronary artery disease risk factors, symptoms of myocardial ischemia, or non-invasive tests indicating ischemia, CAG can confirm the diagnosis.
Radionuclide Imaging
Radionuclide imaging is mainly used for myocardial perfusion imaging to evaluate viable/ischemic myocardium. 99mTc-DPD/PYP/HMDP SPECT bone scintigraphy can detect transthyretin cardiac amyloidosis, and 18F-FDG PET can differentiate cardiac sarcoidosis.
Invasive Hemodynamic Monitoring
Invasive hemodynamic monitoring is used in severe heart failure for assessing hemodynamic status, evaluating heart transplant feasibility, and diagnosing HFpEF. It commonly involves the use of right heart catheterization (Swan-Ganz catheterization) to measure pressures and oxygen content at various sites, and calculate cardiac output (CO), cardiac index (CI), pulmonary capillary wedge pressure (PCWP), and pulmonary resistance. Left heart catheterization and left ventriculography can also measure end-diastolic and end-systolic volumes to calculate EF, CO, CI, and SV.
In patients with exertional dyspnea where non-invasive tests cannot diagnose HFpEF but clinical suspicion remains high, Swan-Ganz catheterization showing PCWP ≥ 15 mmHg or left ventricular end-diastolic pressure (LVEDP) ≥ 16 mmHg at rest, and PCWP ≥ 25 mmHg during stress confirm HFpEF.
6-Minute Walk Test
6-minute walk test is simple, safe, and convenient for assessing exercise tolerance in chronic heart failure patients to evaluate severity and treatment efficacy. Patients walk as quickly as possible in a straight corridor, and the distance covered in 6 minutes is measured. Distances < 150m, 150 - 450m, and > 450m indicate severe, moderate, and mild heart failure, respectively.
Cardiopulmonary Exercise Testing
Cardiopulmonary exercise testing is suitable only for patients with stable chronic heart failure, and is used to assess cardiac function, determine heart transplant feasibility, and guide exercise rehabilitation. Key parameters include peak oxygen consumption and anaerobic threshold.
Diagnosis
The possibility of heart failure should be assessed based on medical history, symptoms, physical examination, ECG, and chest x-ray. The presence and type of heart failure can be confirmed using B-type natriuretic peptide (BNP) testing and echocardiography. Subsequently, the etiology and precipitating factors can be determined, and the severity, prognosis, and presence of complications should be evaluated.
Differential Diagnosis
Pulmonary Diseases
Since dyspnea is the most common symptom of heart failure, heart failure must be differentiated from pulmonary diseases such as chronic obstructive pulmonary disease, bronchial asthma, and pulmonary embolism. Differentiation can be achieved using medical history, cardiac and pulmonary signs, pulmonary function, and imaging tests.
Pericardial Effusion and Constrictive Pericarditis
These conditions can also cause symptoms similar to right heart failure, such as jugular venous distention, hepatomegaly, and lower limb edema. Echocardiography, chest CT, and CMR can aid in differentiation.
Other Causes of Edema
Heart failure should be differentiated from renal edema, hepatic edema, hypoproteinemia, hypothyroidism, and lower limb venous insufficiency. Unlike cardiac edema, non-cardiac edema does not show signs of superior vena cava obstruction, such as jugular venous distention. Routine laboratory tests can assist in differentiation.
Fatigue and reduced exercise tolerance can be caused by anemia, obesity, neuromuscular diseases, and aging. In HFpEF diagnosis, if there are no typical symptoms such as dyspnea and edema, but only non-specific symptoms such as fatigue and muscle weakness, it is essential to assess the impact of heart failure versus other conditions to avoid overdiagnosis of HFpEF.
Treatment
The goals of heart failure treatment are to prevent and delay the progression of heart failure, alleviate symptoms, improve quality of life, enhance long-term prognosis, and reduce mortality and rehospitalization.
General Measures
Lifestyle Management
Patients and their families should receive accurate guidance on disease knowledge and management, including healthy lifestyle choices, avoidance of precipitating factors, regular medication, self-monitoring, and reasonable follow-up plan.
Daily weight monitoring can provide a simple and direct reflection of fluid retention and diuretic effectiveness. Weight changes often precede clinical signs of fluid retention. Severe chronic heart failure patients may experience clinical or subclinical malnutrition, and significant loss of body fat or reduced dry weight is known as cardiac cachexia, often indicating poor prognosis.
Moderate salt restriction can reduce cardiac volume load, but excessive restriction may lead to hyponatremia. Generally, salt restriction is not emphasized for typical heart failure patients, but for refractory or end-stage heart failure patients with diuretic resistance, moderate salt restriction is reasonable.
Patients in the acute stage or with unstable conditions should limit physical activity to reduce cardiac load. Once hemodynamically stable, moderate exercise is beneficial for improving quality of life. An individualized, gradual exercise plan based on cardiopulmonary evaluation is recommended.
Treatment for Etiology and Precipitating Factors
Etiological Treatment
Identifying and treating underlying conditions that may impair cardiac function is crucial for successful treatment.
Elimination of Precipitating Factors
Common precipitating factors include infections, particularly respiratory infections, which require proper anti-infective treatment. Atrial fibrillation with rapid ventricular rate should be managed by controlling the ventricular rate, and if necessary, cardioversion should be performed. It is essential to identify and correct potential thyroid dysfunction, anemia, renal insufficiency, and electrolyte imbalances.
Medication Treatment
Diuretics
Diuretics are effective in controlling fluid retention. They should be used in any type of heart failure when fluid retention is present. Proper dosing is crucial, insufficient doses can lead to fluid retention, exacerbating heart failure symptoms and reducing the efficacy of drugs, while excessive doses can cause volume depletion, increasing the risk of hypotension and renal dysfunction.
Loop diuretics are represented by furosemide, and act on the thick ascending limb of the loop of Henle, promoting sodium and potassium excretion. They are potent diuretics. For mild heart failure, a low dose of 20 mg once daily is generally initiated, gradually increasing until a weight reduction of 0.5 - 1.0 kg/day is achieved. In severe chronic heart failure, doses can be increased to 100 mg twice daily. Intravenous administration is more effective than oral route. Side effects such as hypokalemia should be prevented.
Thiazide diuretics are represented by hydrochlorothiazide, and act on the distal convoluted tubule and the distal part of the loop of Henle, inhibiting sodium reabsorption and consequently potassium reabsorption due to Na+-K+ exchange. They are moderate diuretics and less effective when GFR < 30 ml/min. For mild heart failure, the treatment regimen is initially 12.5 - 25 mg once daily, gradually increasing to 75 - 100 mg per day, in 2 - 3 divided doses. Attention should be paid to electrolyte balance, and they are often in combination with potassium-sparing diuretics. They can inhibit uric acid excretion, causing hyperuricemia, and may affect glucose and lipid metabolism with long-term high doses.
Potassium-sparing diuretics act on the distal convoluted tubule, antagonizing aldosterone or directly inhibiting Na+-K+ exchange to conserve potassium. They have a weak diuretic effect and are often in combination with the above diuretics to enhance diuresis and prevent hypokalemia. Common drugs include spironolactone, triamterene, and amiloride. The treatment regimen includes spironolactone 10 - 20 mg once daily, increasing to 20 - 40 mg; triamterene 25 - 50 mg once daily, increasing to 200 mg; amiloride 2.5 - 5 mg once daily, increasing to 20 mg.
AVP receptor antagonists reduce water reabsorption by binding to V2 receptors without increasing sodium excretion, and can be used in patients with hyponatremia or diuretic resistance. Common drug is tolvaptan, starting at 7.5 - 15 mg once daily, with a maximum dose of 30 mg.
RAAS Inhibitors
Angiotensin-converting enzyme inhibitors (ACEIs) inhibit ACE, reducing ATII production and RAAS activity, improving ventricular remodeling by mitigating adverse neurohormonal compensatory mechanisms.
In HFrEF patients, early and adequate administration can alleviate symptoms, slow progression, and reduce mortality. They are recommended for all HFrEF patients unless contraindicated.
In HFmrEF patients, ACEIs may reduce mortality and hospitalization risk, and should be considered.
In HFpEF patients, evidence for improved prognosis is insufficient, but if hypertension, myocardial infarction, or other indications are present, ACEIs can be considered.
The treatment starts with a low dose, increasing gradually to the target or maximum tolerated dose. Side effects include hypotension, transient renal dysfunction, hyperkalemia, dry cough, and angioedema. ACEIs are contraindicated in angioedema, anuric renal failure, pregnancy, and ACEI allergy; and can be used cautiously in hypotension, bilateral renal artery stenosis, significant creatinine elevation (>265 μmol/L), and hyperkalemia (>5.5 mmol/L). Renal function and potassium should be monitored within 1 - 2 weeks after initiation or dose adjustment, and reviewed regularly.
Angiotensin receptor blockers (ARBs) block ATII from binding to AT1 receptors, inhibiting RAAS without affecting bradykinin degradation. Therefore, dry cough and angioedema are less common. They are preferred in patients intolerant to ACEIs.
Angiotensin receptor neprilysin inhibitors (ARNIs), such as sacubitril/valsartan, inhibit neprilysin to reduce BNP degradation and block AT1 receptors to suppress RAAS overactivation.
In HFrEF patients, ARNIs further reduce hospitalization and cardiovascular mortality, improving symptoms and quality of life. ARNIs are recommended as initial therapy or to replace ACEIs/ARBs if symptoms persist.
In HFmrEF patients, ARNIs may reduce mortality and hospitalization risk, and can be considered.
In HFpEF patients, ARCIs may reduce rehospitalization risk in females and patients with relatively lower LVEF, and can be considered.
The treat starts with a low dose of 50 - 100 mg, increasing every 2 - 4 weeks to a target dose of 400 mg daily, in 2 divided doses.
β-Blockers
β-blockers inhibit sympathetic overactivation, protecting myocardial cells and improving ventricular remodeling.
In HFrEF and HFmrEF patients, long-term use improves left ventricular function, reduces mortality and hospitalization, and significantly lowers sudden death risk. They are recommended for all patients unless contraindicated.
In HFpEF patients, there are limited evidences, and they are not routinely recommended. If there are indications such as coronary artery disease, myocardial infarction, and atrial fibrillation with rapid ventricular rate, they are recommended.
Clinically validated β-blockers include metoprolol, bisoprolol, and carvedilol. They can be used early when hemodynamically stable, with a low dose, gradually increasing to the maximum tolerated dose for maintenance. Contraindications include bronchospastic diseases, severe bradycardia, second-degree or higher AV block, severe peripheral vascular disease (Raynaud disease), and severe acute heart failure. Abrupt discontinuation should be avoided to prevent symptom exacerbation. In chronic heart failure with acute decompensation, the existing β-blocker dose should be maintained if possible unless there is low perfusion or cardiogenic shock.
Mineralocorticoid Receptor Antagonists (MRAs)
MRAs block the effects of aldosterone and inhibit ventricular remodeling, improving prognosis in all types of heart failure. They are recommended for symptomatic chronic heart failure patients.
First-generation MRA spironolactone is most widely used, but can cause gynecomastia in males due to anti-androgen effects. Dosage is 20 - 40 mg daily in 1 - 2 divided doses.
Second-generation MRA eplerenone is a selective MRA with weaker anti-androgen effects, leading to fewer side effects, and is suitable for older patients, diabetic patients, and renal impairment patients. The treatment starts with 25 mg daily, up to 50 mg daily.
Contraindications include serum potassium ≥5.0 mmol/L or estimated glomerular filtration rate (eGFR) ≤30 ml/(min·1.73 m2). Regular monitoring of renal function and potassium is necessary.
Sodium-Glucose Cotransporter 2 Inhibitors (SGLT2i)
SGLT2i inhibit sodium-glucose reabsorption in the renal proximal tubules, promoting urinary glucose and sodium excretion, reducing blood glucose and decreasing volume load. They also improve energy metabolism and endothelial function, and inhibit inflammation and fibrosis, reducing heart failure and cardiovascular mortality risks in type 2 diabetes patients and cardiovascular death and heart failure hospitalization risks in all ejection fraction (EF) types of heart failure. SGLT2i are recommended for all EF types of heart failure.
In stable heart failure patients without contraindications, the treatment regimen is dapagliflozin or empagliflozin 10 mg once daily.
Contraindications include renal impairment [dapagliflozin not for eGFR <30 ml/(min·1.73 m2), empagliflozin not for eGFR <20 ml/(min·1.73 m2)], diabetes, and systolic blood pressure < 95 mmHg. Attention should be paid to euglycemic ketoacidosis and risk of genital and soft tissue infections, and hypovolemia should be prevented.
Digitalis Glycosides
Digitalis glycosides exert pharmacological effects by inhibiting Na+-K+-ATPase:
They enhance myocardial contractility by promoting Ca2+-Na+ exchange in myocardial cells and increasing intracellular Ca2+ concentration.
In therapeutic doses, they inhibit cardiac conduction, mainly at the atrioventricular junction.
They increase cardiac baroreceptor sensitivity, reducing central nervous system excitatory impulses.
They reduce sodium reabsorption and inhibit renin secretion.
Digoxin improves heart failure symptoms and exercise tolerance, and reduces hospitalization but does not significantly affect survival. It is suitable for HFrEF patients with persistent symptoms after administration of diuretics, ACEIs/ARBs/ARNIs, β-blockers, MRAs, and SGLT2i, or symptomatic heart failure with atrial fibrillation and rapid ventricular rate.
The common dose is 0.125 - 0.25 mg daily, and lower dose (0.125 mg every other day) can be given to patients over age 70, with renal impairment, or with low body weight. Is it recommended to maintain serum digoxin concentration at 0.5 - 0.9 μg/L. Overdose can cause arrhythmias, gastrointestinal reactions, and mental symptoms.
Contraindications include sick sinus syndrome, second-degree or higher AV block; acute myocardial infarction (<24 hours), especially with progressive ischemia; Wolff-Parkinson-White syndrome with atrial fibrillation or flutter; and hypertrophic obstructive cardiomyopathy.
Ivabradine
Ivabradine is a selective sinus node If current inhibitor, slowing heart rate and prolonging diastole without affecting cardiac conduction or having negative inotropic effects. It is suitable for chronic heart failure patients with LVEF ≤ 35%, class II-IV, sinus rhythm, and heart rate ≥70 bpm on top of β-blockers.
The dosage is initially 5 mg daily in 2 divided doses, and can be adjusted based on heart rate, up to 15 mg daily in 2 divided doses. The dosage should be reduced or the treatment can be discontinued if resting heart rate drops below 50 bpm or if dizziness and fatigue occur.
Soluble Guanylate Cyclase (sGC) Stimulators
sGC stimulators, such as vericiguat, directly stimulate sGC and stabilize nitric oxide binding, enhancing the NO-sGC-cGMP pathway to improve myocardial and vascular function. The representative drug currently available is vericiguat, and is suitable for recently decompensated heart failure patients with LVEF < 45% after stabilization.
The dosage is initially 2.5 mg once daily, increasing every 2 weeks based on blood pressure, up to 10 mg daily. The dosage should be reduced or the treatment should be discontinued if systolic blood pressure is below 90 mmHg or symptomatic hypotension occurs. It is contraindicated if eGFR <15 ml/(min·1.73 m2).
Vasodilators
Vasodilators are not recommended for chronic heart failure treatment unless concurrent angina or hypertension. They are contraindicated in patients with outflow tract obstruction or severe valvular stenosis.
Non-Medication Treatment
Cardiac Resynchronization Therapy (CRT)
Some heart failure patients experience atrioventricular, interventricular, and (or) intraventricular dyssynchrony, leading to reduced myocardial contractility. CRT improves contraction synchrony, increases cardiac output, alleviates heart failure symptoms, reduces hospitalization rates, and lowers mortality. CRT implantation can be considered in patients in sinus rhythm with persistent heart failure symptoms despite optimal medical therapy for over 3 months, class II-IV, LVEF ≤ 35%, and QRS duration >130 ms. Patients with indications for a standard pacemaker and LVEF ≤ 50% may also consider CRT.
Implantable Cardioverter Defibrillator (ICD)
More than half of moderate to severe heart failure patients die from malignant ventricular arrhythmias leading to sudden cardiac death. ICD can be used for primary prevention in the following patients:
- LVEF still ≤ 35% and class II-III after more than 3 months of optimized medical therapy
- LVEF ≤ 30% and class I 40 days after myocardial infarction and 90 days after revascularization, with optimized medical therapy
ICD can also be used for secondary prevention in heart failure patients who have survived cardiac arrest or have hemodynamically unstable sustained ventricular tachycardia.
Left Ventricular Assist Device (LVAD)
LVAD is suitable for short-term bridging therapy for patients awaiting heart transplantation and as a replacement therapy for end-stage heart failure patients. The miniaturization, precision, and portability of LVADs have been achieved, making them a promising alternative to heart transplantation.
Heart Transplantation
Heart transplantation is currently the ultimate treatment for end-stage heart failure. Accurate assessment of indications for heart transplantation is crucial.