Premature atrial contractions (PACs), also known as atrial premature beats, are atrial activations originating from any location in the atria outside the sinoatrial node, and are a common type of arrhythmia in clinical practice.
Clinical Manifestations
The main symptoms are palpitations and subjective skipped beats, and some patients may experience chest tightness or malaise. However, some individuals may have no symptoms. PACs are often functional, and about 60% of normal adults show PACs on a 24-hour Holter monitor. The incidence of PACs is significantly higher in patients with various organic heart diseases, such as coronary artery disease, pulmonary heart disease, and cardiomyopathy, and they can often cause other tachyarrhythmias.
Electrocardiogram Features
ECG characteristics include:
- Premature P waves with a different morphology from sinus P waves
- PR interval > 120 ms
- Supraventricular QRS complexes, sometimes with aberrant ventricular conduction
- Mostly incomplete compensatory pause
If occurring early in diastole, when the AV node is still refractory from the previous beat, conduction may be blocked, resulting in no QRS complex (called blocked or non-conducted PACs) or slow conduction (prolonged PR interval).
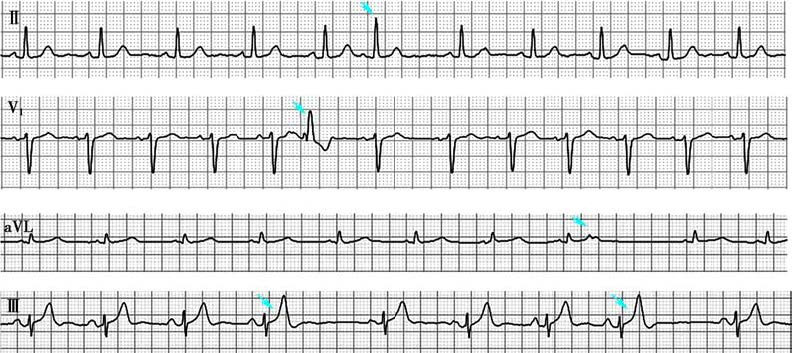
Figure 1 Premature atrial contractions
In lead II, the arrow indicates a PAC; in lead V1, the arrow indicates a PAC with aberrant ventricular conduction; in leads aVL and III, the arrows indicate non-conducted PACs; in lead aVL, the premature atrial P wave partially fuses with the preceding T wave; in lead III, the premature atrial P wave completely fuses with the preceding T wave, resulting in a peaked T wave.
Treatment
PACs typically do not require treatment. Smoking, alcohol consumption, and caffeine can trigger PACs, so patients should be advised to quit or reduce consumption. If symptoms are present or if PACs induce tachycardia, treatment with β-blockers or non-dihydropyridine calcium channel blockers may be considered.