Atrioventricular reentrant tachycardia (AVRT) is a type of tachycardia caused by accessory pathways. Normally, fibrous fatty tissue separates the atria and ventricles, acting as an insulating layer. If this layer is bypassed by subepicardial myocardial fibers, the atrial and ventricular muscles can connect directly, forming an accessory pathway. These pathways can be single or multiple muscle bundles, mainly located around the tricuspid valve annulus on the free wall of the right ventricle, the septal surface of the atrioventricular valve annulus, and the free wall of the left ventricle near the posterior mitral valve. The most common are accessory atrioventricular pathways, also known as Kent bundles. Less common pathways include atriohisian tracts, nodoventricular pathways, and fasciculoventricular pathways, the latter two also known as Mahaim fibers. About 10% of patients have multiple pathways.
Accessory pathways have antegrade (atrial-to-ventricular) and/or retrograde (ventricular-to-atrial) conduction properties. When conduction occurs through the pathway, it can pre-excite the ventricles, showing pre-excitation waves (δ waves on ECG) under sinus rhythm; this is called a manifest pathway or manifest pre-excitation (ventricular pre-excitation). If the pathway only conducts retrogradely, without pre-excitation waves under sinus rhythm, it is called a concealed pathway.
Compared to the normal atrioventricular conduction system, accessory pathways have shorter conduction time and relatively longer refractory period. If an atrial premature beat occurs while the pathway is refractory but the AV node is excitable, conduction occurs antegradely through the AV node and retrogradely through the pathway, forming a reentrant circuit and producing orthodromic AVRT, where the QRS complex is normal. In manifest pre-excitation, when conduction occurs antegradely through the pathway and retrogradely through the AV node, it results in antidromic AVRT, presenting wide QRS tachycardia, which must be distinguished from ventricular tachycardia.
When ventricular pre-excitation leads to AVRT, it is called pre-excitation syndrome. The most common type, caused by Kent bundles, is Wolff-Parkinson-White (WPW) syndrome, also known as typical pre-excitation syndrome. Other rare pathways cause variant pre-excitation syndromes. When pre-excitation is in combination with atrial fibrillation (AF) or atrial flutter, the rapid atrial rate can cause an extremely fast ventricular rate; in some patients with short refractory periods in the pathway, all impulses may conduct through the pathway, with heart rates exceeding 300 beats per minute, potentially leading to ventricular fibrillation.
Etiology
Most patients do not have other cardiac abnormalities. AVRT can be detected at any age during routine ECG or tachycardia episodes. It is occasionally seen with congenital heart diseases such as Ebstein anomaly, mitral valve prolapse, and various cardiomyopathies.
Clinical Manifestations
The clinical manifestations are similar to AVNRT. The severity of symptoms depends on the heart rate during tachycardia, duration, type, and any underlying heart disease. When pre-excitation is in combination with atrial fibrillation or flutter, it can lead to hemodynamic instability, such as amaurosis fugax, syncope, and even Stokes-Adams attacks.
Electrocardiogram Features
AVRT
The ECG shows continuous, rapid, regular QRS complexes with a rate of 150 - 220 beats per minute, usually without distinct P waves. Most QRS complexes appear normal; however, some may show wide, abnormal QRS complexes, known as wide QRS tachycardia. Orthodromic AVRT typically presents tachycardia with normal QRS morphology, which is the most common type, accounting for over 90% of AVRT cases. Antidromic AVRT presents wide QRS tachycardia. In rare cases, orthodromic AVRT with bundle branch block or intraventricular aberrant conduction can also present wide QRS tachycardia. When pre-excitation is in combination with atrial fibrillation (AF) or atrial flutter, impulses conduct through both the accessory pathway and the AV node, resulting in tachycardia with variable QRS morphology, which can be normal or wide.
Ventricular Pre-excitation
ECG shows:
- PR intervals less than 0.12 seconds
- Slurred initial part of the QRS complexes (δ waves), with normal terminal portion
- Secondary changes in ST-T waves, opposite to the main direction of the QRS complexes
Based on the main direction of the QRS complex in chest leads, pre-excitation is classified as type A and type B.
In type A, all chest lead QRS complexes are upright, while in type B, V1, V2 leads are downward, while V4 to V6 leads are upward.

Figure 1 Orthodromic AVRT
Continuous, rapid, regular QRS complexes with normal morphology and duration, at a rate of 200 beats per minute, without distinct P waves

Figure 2 Antidromic AVRT
Continuous, rapid, regular QRS complexes with wide and abnormal morphology, QRS duration of 0.13 seconds, at a rate of 214 beats per minute
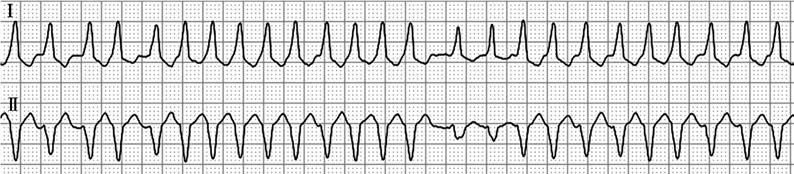
Figure 3 Pre-excitation with atrial fibrillation
Irregular RR intervals, variable QRS morphology with pre-excitation waves at the onset, ventricular rate of 201 beats per minute
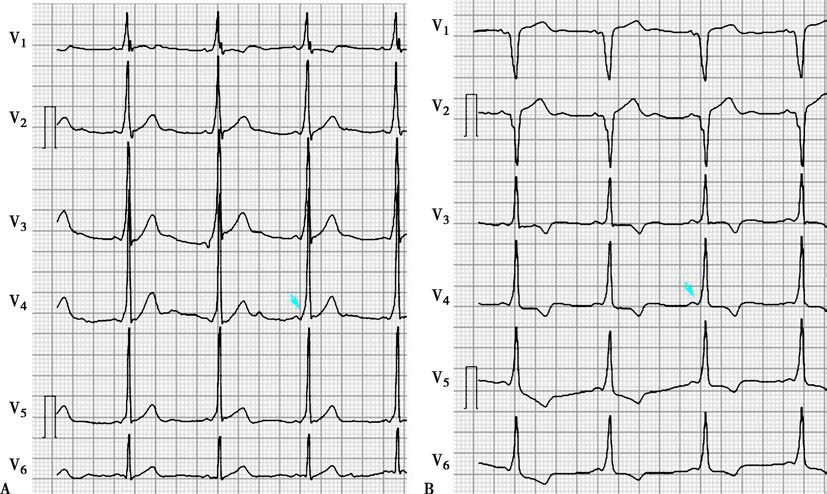
Figure 4 Ventricular pre-excitation
A. Type A pre-excitation; B. Type B pre-excitation, with arrows indicating δ wave
Electrophysiological Study
Electrophysiological study can confirm the diagnosis, locate the accessory pathway, and guide catheter ablation treatment. Most accessory pathways conduct rapidly (except atypical pathways) and have electrophysiological characteristics different from normal AV conduction. They are similar to ordinary myocardial tissue and are fast-response cells, with rapid and fixed conduction and lacking decremental conduction.
Characteristics include:
- All-or-nothing conduction (the conduction time of the pathway does not gradually extend with earlier ventricular stimulation, showing a relatively fixed VA interval until the pathway enters the refractory period, preventing ventricular pacing from retrogradely conducting to the atria, resulting in sudden loss of A waves)
- Earliest retrograde atrial activation during ventricular pacing (because the pathway conducts faster than the AV node, allowing rapid atrial activation through the pathway)
Indications for electrophysiological study include:
- Assisting in diagnosis
- Determining the location and number of pathways
- Assessing whether pathways directly participate in the reentrant circuit during tachycardia or act as bystanders
- Evaluating the maximum ventricular rate during atrial fibrillation or flutter
- Assessing the effectiveness of treatments such as medication, catheter ablation, and surgery
- Risk stratification of manifest pathways
Treatment
For acute orthodromic AVRT, management can follow the approach for AV nodal reentrant tachycardia (AVNRT). In antidromic AVRT, if vagal stimulation and adenosine are ineffective, intravenous administration of ibutilide, procainamide, flecainide, or propafenone can be considered.
In patients with pre-excitation and atrial fibrillation or atrial flutter, the first choice for terminating tachycardia is electrical cardioversion, or intravenous ibutilide or propafenone. β-blockers, verapamil, diltiazem, digitalis glycosides, and amiodarone are contraindicated as they may inhibit AV node conduction, enhancing accessory pathway conduction and increasing the risk of ventricular fibrillation.
If hemodynamic instability occurs or if medication fails to convert or control the tachycardia, electrical cardioversion is indicated.
Catheter ablation is the preferred treatment for curing AVRT. It is especially recommended for patients with frequent tachycardia episodes or those with concomitant atrial fibrillation or atrial flutter, and should be performed early.
In patients with pre-excitation but no history of tachycardia, the decision to proceed with catheter ablation should be based on whether patients are in a high-risk occupation and electrophysiological study risk stratification. If patients are in a high-risk occupation or the study indicates a high-risk accessory pathway, early catheter ablation is advised.