Premature ventricular contractions (PVCs), also known as ventricular premature beats, are the most common arrhythmia. It is premature beats originating from an ectopic focus in the ventricles below the His bundle.
Etiology
PVCs are commonly seen in various organic heart diseases, such as hypertension, coronary artery disease, cardiomyopathy, myocarditis, and valvular heart disease. They can also occur in individuals with normal cardiac structure and function, and are triggered by emotional stress, excessive fatigue, excessive smoking, alcohol or caffeine intake, and electrolyte imbalances. Certain medications, such as digitalis glycosides, quinidine, tricyclic antidepressants, and antineoplastic drugs, can also cause PVCs.
Clinical Manifestations
The severity of symptoms from PVCs is not directly related to their frequency. Patients generally experience palpitations, chest tightness, sensation of weightlessness, or strong heartbeats following compensatory pauses. Symptoms may include dizziness and malaise. In patients with severe organic heart disease, frequent PVCs over a prolonged period can lead to angina, hypotension, or heart failure. During auscultation, a longer pause may be noted after the premature beat, with a weakened second heart sound and only audible first heart sound, and weakened or absent radial pulse.
Electrocardiogram Features
ECG shows:
- Premature, wide, and abnormal QRS complexes, typically exceeding 0.12 seconds in duration
- T wave direction opposite to the main QRS complex
- Constant interval between the PVC and the preceding sinus beat (coupling interval), often followed by a complete compensatory pause

Figure 1 Premature ventricular contractions
The 3rd and 8th QRS complexes occur prematurely, with widened and abnormal QRS complexes, no preceding P wave, and are followed by a complete compensatory pause.
Types of PVCs
PVCs can occur in isolation or regularly. When a PVC follows every sinus beat, it is called bigeminy; when it follows every two sinus beats, it is called trigeminy. Two consecutive PVCs are termed couplets, and three or more consecutive PVCs are termed ventricular tachycardia. If a PVC occurs between two sinus beats without causing a pause, it is called interpolated PVC. In the same lead, PVCs with identical morphology are called monomorphic PVCs, while those with different morphologies are called polymorphic or multiform PVCs.
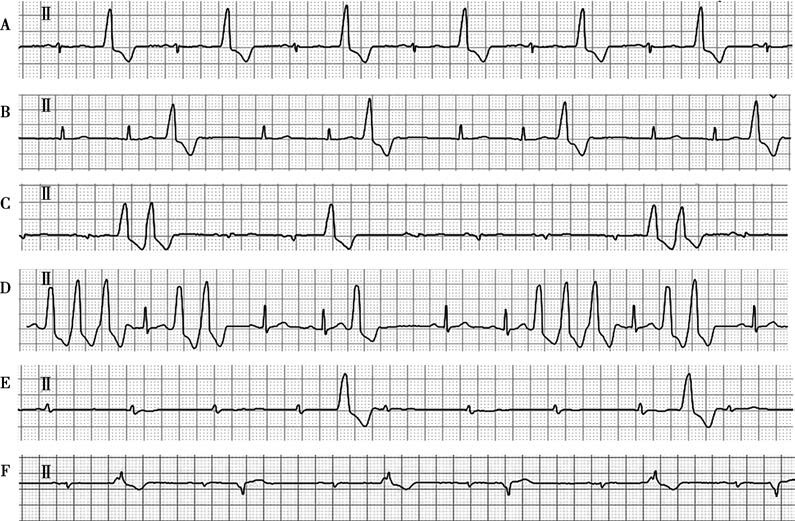
Figure 2 Types of premature ventricular contractions
A. Bigeminy: A PVC follows each sinus beat.
B. Trigeminy: A PVC follows every two sinus beats.
C. Couplets: The 3rd and 4th QRS complexes appear consecutively.
D. Short run of ventricular tachycardia: The 1st, 2nd, and 3rd QRS complexes appear consecutively.
E. Interpolated PVC: The 5th and 10th QRS complexes occur prematurely without a compensatory pause.
F. Polymorphic PVCs: The 2nd and 4th QRS complexes have different morphologies.
Treatment
A comprehensive assessment of the type of PVCs, symptoms, and any underlying heart disease should be conducted. Treatment decisions should be based on the clinical situation, and a rational and effective treatment plan should be developed.
Without Organic Heart Disease
PVCs do not increase the risk of cardiac death in these patients. If patients have no significant symptoms or only mild symptoms, medication is not necessary. If symptoms are significant, treatment should aim to alleviate them. It is important to provide patients with reassurance about the benign prognosis to reduce anxiety and stress. Triggers such as smoking, coffee/tea, anxiety, and stress should be avoided. β-blockers, non-dihydropyridine calcium channel blockers, or propafenone can be administrated.
With Organic Heart Disease
In patients with organic heart disease and heart failure, the primary focus should be on treating the heart disease itself, without necessarily using medication for PVCs. If symptoms are significant, β-blockers and amiodarone can be used. In case of acute myocardial ischemia with PVCs, reperfusion therapy is the first choice, and prophylactic use of antiarrhythmic drugs is not recommended. If frequent or multiform PVCs occur before reperfusion therapy, β-blockers can be used. The underlying causes, especially electrolyte imbalances such as hypokalemia and hypomagnesemia, should be addressed. Class Ia and Ic antiarrhythmic drugs should be avoided due to their proarrhythmic effects, which may increase overall mortality and the risk of sudden death.
Catheter Ablation
For frequent PVCs originating from the right ventricular outflow tract or left ventricular posterior septum, if symptoms are significant and antiarrhythmic drugs are ineffective or not tolerated, and there is no significant organic heart disease, catheter ablation can be considered, as it has a high success rate. For monomorphic PVCs originating from other locations, catheter ablation is also an option, though with a lower success rate.