Ventricular tachycardia (VT) originates from the specialized conduction system below the bundle of His or from ventricular myocardium, and is characterized by three or more consecutive ectopic beats. Prompt and accurate diagnosis and treatment of VT are clinically significant.
Etiology
VT often occurs in patients with various organic heart diseases. The most common cause is coronary artery disease, followed by cardiomyopathy, heart failure, and valvular heart disease. Other causes include metabolic disorders, electrolyte imbalances, and digitalis toxicity. VT can occasionally occur in those without organic heart disease, which is known as idiopathic VT, often originating from the right ventricular outflow tract (RVOT), left ventricular septum, or aortic sinus. A small proportion of VTs are related to genetic factors, which is known as channelopathies, such as long QT syndrome and Brugada syndrome.
Clinical Manifestations
The symptoms of VT vary based on the ventricular rate during episodes, duration, underlying heart disease, and cardiac function. Non-sustained VT (lasting less than 30 seconds and self-terminating) may present with no significant symptoms. Sustained VT (lasting more than 30 seconds, requiring medication or cardioversion) is often associated with significant hemodynamic instability and myocardial ischemia, with symptoms including hypotension, dizziness, dyspnea, angina, and syncope. Some episodes of polymorphic VT or Torsades de Pointes may rapidly degenerate into ventricular fibrillation, leading to cardiogenic syncope, cardiac arrest, and sudden death.
Auscultation may reveal a mildly irregular rhythm, splitting of the first and second heart sounds, and systolic blood pressure variations with heartbeats.
Electrocardiographic Features
ECG shows:
- Three or more consecutive PVCs
- Ventricular rate of typically 100 - 250 bpm
- Regular or slightly irregular rhythm
- Atrioventricular dissociation with independent atrial activity and no fixed relationship to QRS complexes
- Occasional retrograde ventricular capture of the atria
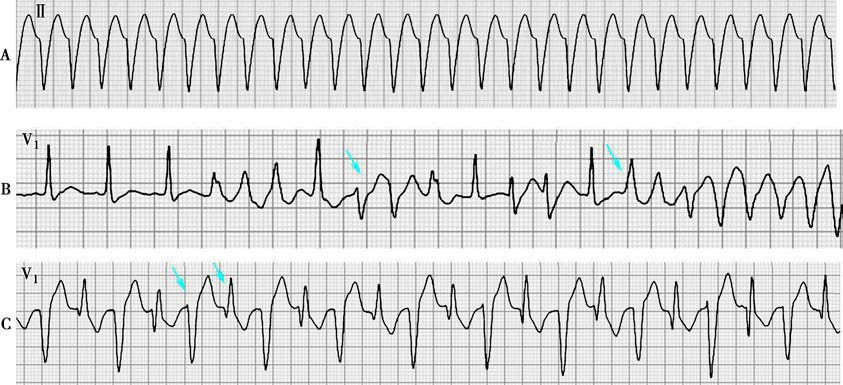
Figure 1 Ventricular tachycardia
A. Lead II shows a series of rapid, wide, abnormal QRS complexes with a uniform morphology and slightly irregular RR intervals.
B. Lead V1 shows QRS complexes with varying morphologies, indicating polymorphic VT.
C. Lead V1 shows alternating upward and downward QRS main wave directions, indicating bidirectional VT.
Ventricular Capture and Fusion Beats
During VT, some supraventricular impulses can be conducted to the ventricles, resulting in ventricular capture, seen as a normal QRS complex occurring prematurely after a P wave. Fusion beats have QRS morphology between sinus and ectopic ventricular beats, indicating partial ventricular capture. The presence of ventricular capture and fusion beats is crucial for diagnosing VT. VT can be classified into monomorphic VT and polymorphic VT based on QRS morphology; bidirectional VT is characterized by alternating QRS axis directions. The ECG presentations of ventricular tachycardia and supraventricular tachycardia with wide QRS complexes are very similar, but their clinical significance and management differ greatly, so careful differentiation is required.

Table 1 Differential diagnosis of wide QRS tachycardia
Electrophysiological Study
Electrophysiological study is valuable for diagnosing VT and determining its origin. If His bundle waves (H) can be recorded during tachycardia, analyzing the interval from the start of the His wave to the start of the ventricular wave (HV interval) helps differentiate between supraventricular and ventricular tachycardia. In supraventricular tachycardia, the HV interval should be greater than or equal to that during sinus rhythm, while in VT, the HV interval is shorter than the sinus HV interval or negative (due to retrograde conduction through the His-Purkinje system).
Treatment
The treatment principles for ventricular tachycardia are as follows:
- For non-sustained VT in patients without organic heart disease, if asymptomatic or without hemodynamic impact, management is similar to that for premature ventricular contractions.
- For those with organic heart disease or a clear trigger, targeted treatment should be administered first.
- Sustained VT requires treatment regardless of the presence of organic heart disease.
Termination of VT Episodes
For VT without significant hemodynamic compromise, intravenous amiodarone, lidocaine, or procainamide can be used to terminate the episode. If medications are ineffective or if patients experience hypotension, shock, angina, heart failure, or cerebral hypoperfusion, immediate direct current cardioversion is necessary. After successful cardioversion, intravenous amiodarone or lidocaine can be administered to prevent short-term recurrence. VT caused by digitalis toxicity should be treated with medication rather than electrical cardioversion.
Prevention of Recurrence
Efforts should be focused on identifying and treating reversible factors that trigger and sustain VT, such as myocardial ischemia, hypotension, and hypokalemia. Treating heart failure can help reduce VT episodes. In case of sinus bradycardia or atrioventricular block where the ventricular rate is too slow, ventricular arrhythmias may be induced, and treatment with atropine or a pacemaker may be necessary.
In patients with acute myocardial ischemia and VT, coronary revascularization is preferred, and β-blockers can be used to prevent ventricular arrhythmias. β-blockers reduce the risk of sudden death after myocardial infarction, primarily by decreasing sympathetic activity and improving myocardial ischemia. In patients with ventricular fibrillation or hemodynamically unstable VT due to irreversible causes occurring more than 48 hours after acute myocardial infarction, an implantable cardioverter-defibrillator (ICD) may be considered.
ICD implantation is suitable for patients with sustained polymorphic VT and those with genetic arrhythmia syndromes. Patients with recurrent monomorphic VT despite medication or frequent ICD shocks may consider catheter ablation therapy.