Interstitial lung disease (ILD), also known as diffuse parenchymal lung disease (DPLD), is a group of diffuse lung diseases primarily affecting the lung interstitium and alveolar spaces, leading to the loss of alveolar-capillary functional units. Clinically, it is characterized by progressively exacerbated dyspnea, restrictive ventilatory dysfunction with reduced diffusion capacity, hypoxemia, and diffuse bilateral lung lesions on imaging. ILD can ultimately progress to diffuse pulmonary fibrosis and honeycomb lung, leading to respiratory failure and death.
ILD comprises over 200 acute and chronic pulmonary diseases, including both common and rare conditions, with most having unclear etiologies. Based on etiology, clinical manifestations, and pathological features, ILD can be classified into the following categories:
- ILD with known causes
- Idiopathic interstitial pneumonias (IIP)
- Granulomatous ILD
- Other rare ILDs
Idiopathic interstitial pneumonias are a group of interstitial lung diseases with unknown causes. IIP can be classified into three major groups:
- Major idiopathic interstitial pneumonias
- Rare idiopathic interstitial pneumonias
- Unclassified idiopathic interstitial pneumonias
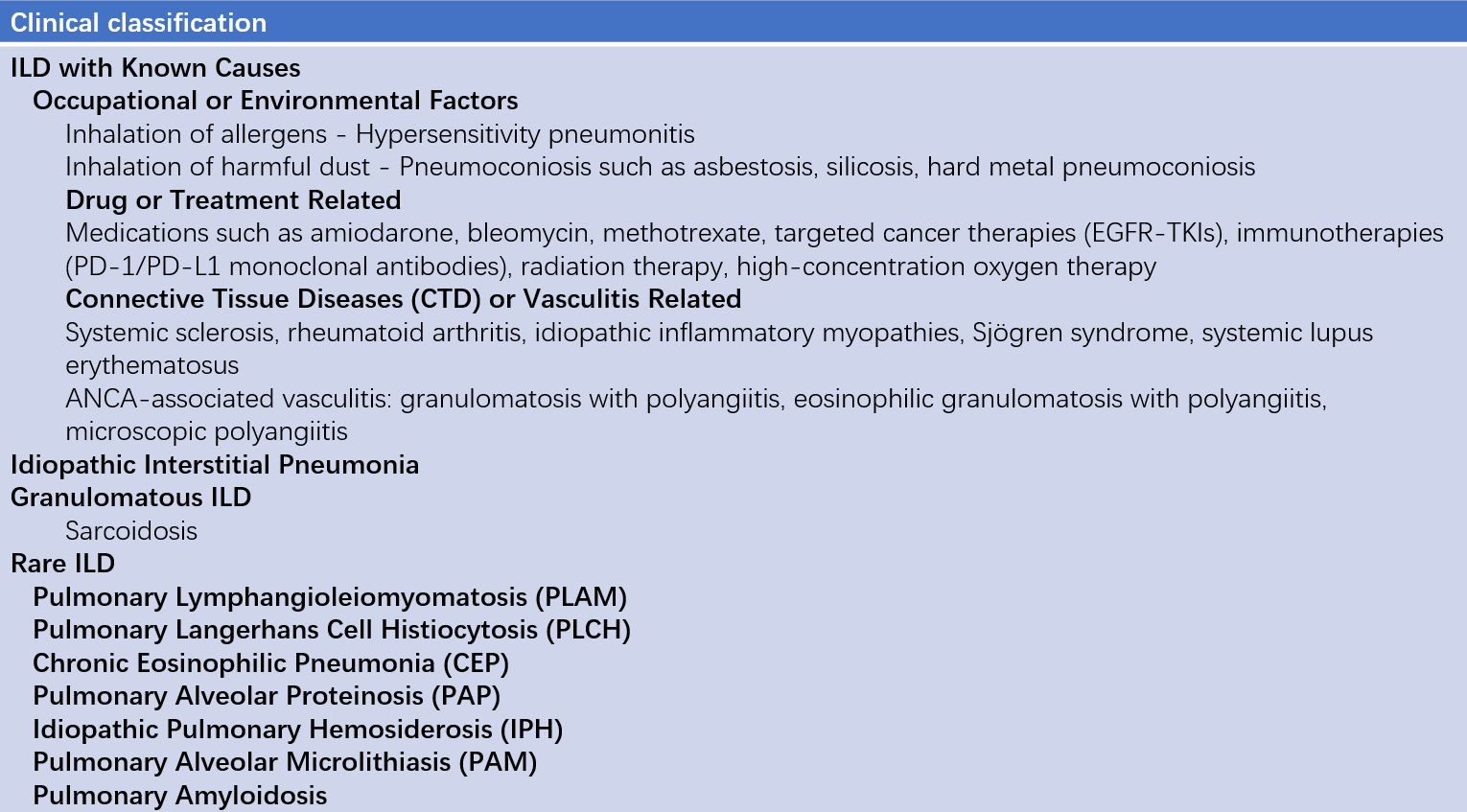
Table 1 Classification of interstitial lung disease (ILD)
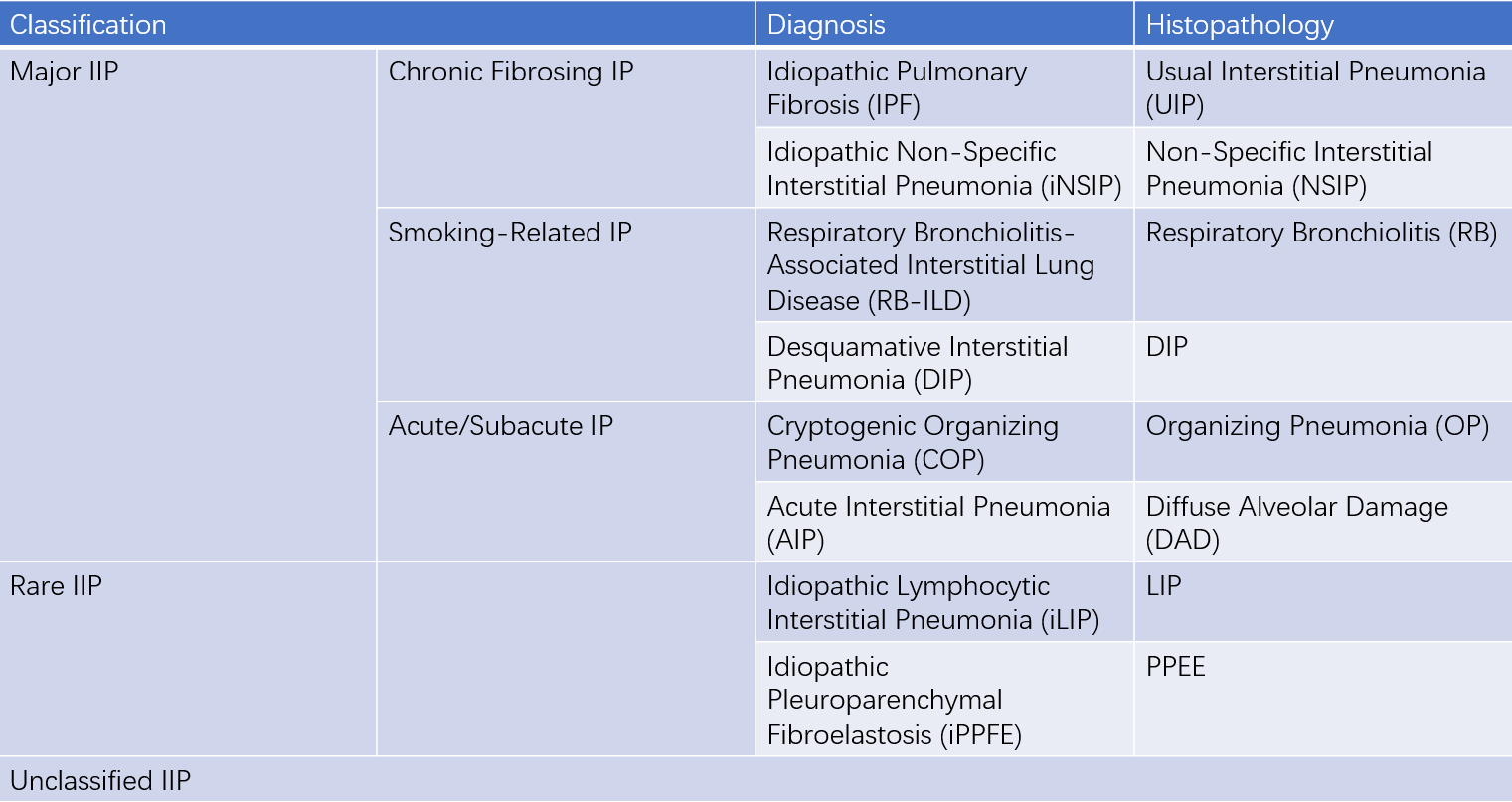
Table 2 Classification of idiopathic interstitial pneumonia (IIP)
Diagnosis
Diagnosing a specific interstitial lung disease (ILD) is a dynamic process that requires close collaboration in clinicians, radiologists, and pathologists to verify or revise previous diagnoses based on comprehensive data.
Clinical Manifestations
Different ILDs have varying clinical presentations, often with insidious onset. The most common symptom is dyspnea and (or) tachypnea, initially occurring during exertion and progressively exacerbated as the disease advances. Persistent dry cough is also common, while hemoptysis, thoracodynia, and wheezing are less common. Systemic symptoms such as fever, rash, myalgia, arthralgia, joint swelling, xerostomia, and xerophthalmia may suggest underlying connective tissue diseases.
Important medical history includes connective tissue diseases, cancer, organ transplants, and heart disease; medication history, especially drugs that can induce pulmonary fibrosis such as amiodarone, methotrexate, anti-tumor targeted therapy (EGFR-TKI), and immunotherapy (PD-1/PD-L1 monoclonal antibodies); family history of pulmonary fibrosis; smoking history, including the number of cigarettes per day, duration of smoking, and cessation time; occupational or household exposure history, and contact with birds or moldy environments. Understanding these histories is crucial for determining the cause of ILD.
Fine dry crackles or Velcro crackles heard at the end of inspiration at the lung bases are common signs of ILD, especially idiopathic pulmonary fibrosis (IPF), and are early signs.
Clubbed fingers are a common sign in ILD patients, usually indicating long-term lung structural damage and impaired lung function, frequently seen in IPF.
In the late stage of ILD, pulmonary hypertension and cor pulmonale can occur, presenting with cyanosis, tachypnea, P2 > A2, and lower limb edema.
Rashes, joint swelling, and deformities may suggest connective tissue diseases.
Imaging
Most ILD patients show diffuse infiltrative opacities on chest x-ray, but these are not diagnostic. Normal chest x-ray cannot be used to exclude ILD. High-resolution CT (HRCT) provides a detailed view of the extent and nature of parenchymal abnormalities and can detect lesions invisible on x-ray, making it an essential tool for diagnosing ILD. HRCT findings in ILD include reticular opacities, honeycomb opacities, diffuse micronodules, traction bronchiectasis, ground-glass opacities, alveolar consolidation, interlobular septal thickening, subpleural lines, and cystic lesions.
Pulmonary Function Test
ILD patients typically exhibit restrictive ventilatory dysfunction and impaired gas exchange. Restrictive dysfunction is characterized by reduced total lung capacity (TLC), vital capacity (VC), and forced vital capacity (FVC), with decreased lung compliance. The forced expiratory volume in one second/forced vital capacity (FEV1/FVC) ratio is normal or increased. Gas exchange impairment is indicated by reduced diffusing capacity for carbon monoxide (DLCO), increased alveolar-arterial oxygen gradient [P(A-a)O2], and hypoxemia at rest or during exercise.
Laboratory Test
Routine tests include complete blood count, urinalysis, biochemistry, liver and kidney function, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) tests. Tests for autoantibodies related to connective tissue diseases, such as rheumatoid factor (RF), antinuclear antibody (ANA), antineutrophil cytoplasmic antibody (ANCA), anti-cyclic citrullinated peptide antibody, and myositis antibodies, are also performed. Tests for cytomegalovirus (CMV) or pneumocystis (opportunistic infections) and tumor cells (suspected cancer) may be conducted as needed, providing clues to the etiology or associated diseases in ILD.
Bronchoscopy
Bronchoscopy with bronchoalveolar lavage (BAL) and (or) transbronchial lung biopsy (TBLB) and (or) transbronchial lung cryobiopsy (TBLC) is helpful in understanding the nature of diffuse pulmonary infiltrative lesions and differentiating ILD types. Normal bronchoalveolar lavage fluid (BALF) cytology shows macrophages > 85%, lymphocytes ≤ 7% - 15%, neutrophils ≤ 3%, and eosinophils ≤ 1%. Increases in lymphocytes, eosinophils, or neutrophils in BALF have specific clinical significance and can help narrow differential diagnoses. TBLB samples are often too small to diagnose specific ILD types. TBLC, which can obtain larger lung tissue samples, provides better observation of structural changes in the lungs and offers promising clinical application prospects for ILD diagnosis and classification.
Surgical Lung Biopsy
Surgical lung biopsy, including open lung biopsy (OLB) and video-assisted thoracoscopic surgical lung biopsy (VATS-SLB), is usually required to clarify pathological changes and confirm a diagnosis in ILD when clinical data, HRCT features, and even BAL and TBLB/TBLC cannot provide a definitive diagnosis.
To be continued